

The History of Botulinum Toxin
The history of Botulinum Toxin, often referred to as “botox”, is a fascinating journey that spans over several decades. This potent neurotoxin, produced by the bacterium Clostridium botulinum, has found its place in the world of cosmetic dermatology, offering a non-surgical solution to a variety of aesthetic concerns.
The discovery of Botulinum Toxin dates back to the 19th century when a German physician, Justinus Kerner, first identified it while investigating a series of food poisoning cases. Kerner coined the term “botulism” from the Latin word for sausage, “botulus,” as the affected individuals had consumed improperly prepared sausages. He was the first to recognize the paralytic symptoms of botulism and postulated the existence of a “fatty poison” that interfered with the transmission of nerve impulses.
In the early 20th century, Emile Pierre van Ermengem, a Belgian bacteriologist, isolated the bacterium we now know as Clostridium botulinum. He discovered that the bacterium produced a toxin that caused the symptoms of botulism. This marked the first step in understanding the nature of this potent neurotoxin.
Do you want to visit Haridwar? travel agents in Haridwar is the right place to plan your tour. You can book your tour from here.
The therapeutic potential of Botulinum Toxin was not realized until the mid-20th century. During the 1940s and 1950s, scientists at the United States Army’s biological warfare laboratories at Fort Detrick, Maryland, conducted extensive research on Botulinum Toxin as a potential biological weapon. Although the military applications of the toxin were never fully realized, this research paved the way for understanding the toxin’s therapeutic potential.
In the 1960s, Dr. Alan B. Scott, an ophthalmologist, began investigating the potential use of Botulinum Toxin to treat strabismus (crossed eyes), a condition that was difficult to treat surgically. His research led to the development of a purified and diluted form of the toxin that could be injected into muscles to cause temporary paralysis. In 1989, the U.S. Food and Drug Administration (FDA) approved the use of Botulinum Toxin type A (marketed as Botox) for the treatment of strabismus and blepharospasm (uncontrolled blinking).
The cosmetic applications of Botulinum Toxin were discovered somewhat serendipitously. Jean Carruthers, a Canadian ophthalmologist, noticed that her patients who received Botox treatments for eye disorders also experienced improvement in facial wrinkles. This observation led to a series of studies conducted by Jean and her husband, Alastair Carruthers, a dermatologist, which eventually led to the FDA approval of Botox for cosmetic use in 2002.
Do you want to visit char dham? char dham tour operator is the right place to plan you Char Dham tour. You can book you tour from here.
Since then, the use of Botulinum Toxin in cosmetic dermatology has skyrocketed. It is now used to treat a variety of conditions, including forehead wrinkles, crow’s feet, and frown lines. The toxin works by blocking the nerve signals to the muscles, causing them to relax and reducing the appearance of wrinkles.
The journey of Botulinum Toxin from a deadly poison to a beloved wrinkle reducer is a testament to the power of scientific research and innovation. As our understanding of this potent neurotoxin continues to grow, so too will its applications in cosmetic dermatology and beyond.
Different Botulinum Toxins
BOTOX Cosmetic (onabotulinumtoxinA):

Indication
This drug is used in adults for temporary improvement in the appearance of moderate to severe glabellar lines (lines between the eyebrows) associated with corrugator and/or procerus muscle activity. It is also indicated for the treatment of moderate to severe lateral canthal lines (crow’s feet) associated with orbicularis oculi activity, and moderate to severe forehead lines associated with frontalis muscle activity.
Dilution
This drug is supplied in single-dose 50 Units and 100 Units per vial. It should be reconstituted with sterile, preservative-free 0.9% Sodium Chloride Injection USP to obtain a solution at a concentration of 4 Units/0.1 mL. The reconstituted BOTOX Cosmetic should be clear, colorless, and free of particulate matter. It should be administered within 24 hours after reconstitution and stored in a refrigerator during this time period. The vials are for single-dose only.
Administration
The drug is administered intramuscularly into five sites, two each corrugator muscle and one in the procerus muscle for a total dose of 20 Units. The dosage for simultaneous treatment with lateral canthal lines is 64 Units, comprised of 20 Units for forehead lines, 20 Units for glabellar lines, and 24 Units for lateral canthal lines. The drug should be administered no closer than 1 cm above the central eyebrow to reduce the risk of ptosis.
Storage
The product is supplied as a vacuum-dried powder in single-dose vials of 50 or 100 Units. Unopened vials should be stored in a refrigerator (2° to 8°C). Reconstituted BOTOX Cosmetic should also be stored in a refrigerator and used within 24 hours.
Do you want to visit Indiar? tour operator in India is the right place to plan your tour. You can book your tour from here.
DYSPORT (abobotulinumtoxinA):

Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with procerus and corrugator muscle activity in adults less than 65 years of age.
Dilution
This drug is supplied as a dry powder in single-dose 300 Unit and 500 Unit vials. It should be reconstituted with preservative-free 0.9% Sodium Chloride Injection, USP using aseptic technique. The reconstituted DYSPORT should be a clear, colorless solution, free of particulate matter. It should be used for only one injection session and for only one patient. Once reconstituted, it can be stored in a refrigerator, protected from light for up to 24 hours until time of use.
Administration
The dose for the treatment of glabellar lines in adults is a total of 50 Units given intramuscularly in five equal aliquots of 10 Units each to achieve clinical effect. The drug should be administered no more frequently than every three months. To reduce the risk of ptosis, the drug should be injected at least 1 centimeter above the bony supraorbital ridge and no closer than 1 centimeter above the central eyebrow.
Storage
This is supplied as a sterile, lyophilized powder in a single-dose, glass vial. Unopened vials must be stored refrigerated (2°C to 8°C) and protected from light.
XEOMIN (incobotulinumtoxinA):

Indication
It is indicated for temporary improvement in the appearance of moderate to severe glabellar lines with corrugator and/or procerus muscle activity.
Dilution
It should be reconstituted with only 2.5mL sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 4 Units/0.1 mL. The frequency of XEOMIN treatments should be no sooner than every 12 weeks.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 20 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied in single-dose vials of 50, 100, or 200 Units. Unopened vials can be stored at room temperature (20°C to 25°C), in a refrigerator (2°C to 8°C), or a freezer (-20°C to -10°C). Reconstituted XEOMIN should not be used if the solution appears cloudy or contains particulate matter, and any unused solution should be discarded after 24 hours.
JEUVEAU (prabotulinumtoxinA-xvfs):
Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients.
Dilution
This drug is supplied in a single-dose 100 Unit vial. It should be reconstituted with only 2.5mL sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 4 Units/0.1 mL. The reconstituted JEUVEAU should be clear, colorless, and free of particulate matter. It should be administered within 24 hours after reconstitution and stored in a refrigerator during this time period. The vials are for single-dose only.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 20 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied as a vacuum-dried powder in a single-dose vial of 100 Units. Unopened vials should be stored in a refrigerator (2° to 8°C) and protected from light.
DAXXIFY (daxibotulinumtoxinA-lanm)

Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients.
Dilution
This drug is supplied in single-dose 50 Unit and 100 Unit vials. It should be reconstituted with the required amount of sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 8 Units/0.1 mL. The reconstituted DAXXIFY solution should be clear to slightly opalescent and colorless and free of particulate matter. It should be administered within 72 hours after reconstitution and stored in a refrigerator during this time period.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 40 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied as a sterile lyophilized powder in single-dose vials of 50 or 100 Units. Unopened vials should be stored at room temperature (20°C to 25°C) or refrigerated (2°C to 8°C) and protected from light.
General Contraindications
Botulinum toxin drugs are contraindicated in patients with:
Known hypersensitivity to any botulinum toxin products or to any of the components in the formulation. This includes specific hypersensitivity to cow’s milk protein, which may be present in trace amounts in some formulations.
Presence of infection at the proposed injection site(s).
These contraindications apply to all the mentioned botulinum toxin drugs: BOTOX Cosmetic, DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY.
Warnings and Precautions
Lack of Interchangeability between Botulinum Toxin Products
The potency units of botulinum toxin products, including BOTOX Cosmetic (onabotulinumtoxinA), DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY (daxibotulinumtoxinA-lanm), are specific to the preparation and assay method utilized. They are not interchangeable with other preparations of botulinum toxin products. Therefore, units of biological activity of these products cannot be compared to nor converted into units of any other botulinum toxin products assessed with any other specific assay method.
Spread of Toxin Effect:
Postmarketing safety data from botulinum toxin products, including BOTOX Cosmetic, DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY, suggest that botulinum toxin effects may, in some cases, be observed beyond the site of local injection. The symptoms are consistent with the mechanism of action of botulinum toxin and may include asthenia, generalized muscle weakness, diplopia, blurred vision, ptosis, dysphagia, dysphonia, dysarthria, urinary incontinence, and breathing difficulties.
These symptoms have been reported hours to weeks after injection. Swallowing and breathing difficulties can be life-threatening, and there have been reports of death related to the spread of toxin effects. Patients should be advised to seek immediate medical care if swallowing, speech, or respiratory difficulties occur. Although no serious adverse reactions of distant spread of toxin effect associated with these products have been reported in clinical studies for their specific approved indications, these reactions are possible.
Serious adverse reactions with unapproved use:
Serious adverse reactions, including excessive weakness, dysphagia, and aspiration pneumonia, with some adverse reactions associated with fatal outcomes, have been reported in patients who received botulinum toxin injections for unapproved uses. These adverse reactions were not necessarily related to distant spread of toxin, but may have resulted from the administration of botulinum toxin products to the site of injection and/or adjacent structures. In several cases, patients had pre-existing dysphagia or other significant disabilities. There is insufficient information to identify factors associated with an increased risk for adverse reactions associated with the unapproved uses of botulinum toxin products. The safety and effectiveness of botulinum toxin for unapproved uses have not been established.
Hypersensitivity Reactions:
Serious and/or immediate hypersensitivity reactions have been reported for botulinum toxin products. These reactions include anaphylaxis, serum sickness, urticaria, soft tissue edema, and dyspnea. If such a reaction occurs, further injection of the botulinum toxin product should be discontinued and appropriate medical therapy immediately instituted. The use of botulinum toxin products in patients with a known hypersensitivity to any botulinum neurotoxin or to any of the components in the formulation could lead to a life-threatening allergic reaction.
Cardiovascular System:
There have been reports following administration of botulinum toxins of adverse events involving the cardiovascular system, including arrhythmia and myocardial infarction, some with fatal outcomes. Some of these patients had risk factors including pre-existing cardiovascular disease. Use caution when administering to patients with pre-existing cardiovascular disease.
Increased Risk with Pre-Existing Neuromuscular Disorders:
Individuals with peripheral motor neuropathic diseases, amyotrophic lateral sclerosis, or neuromuscular junction disorders (e.g., myasthenia gravis or Lambert-Eaton syndrome) should be monitored particularly closely when given botulinum toxin. Patients with neuromuscular disorders may be at increased risk of clinically significant effects including generalized muscle weakness, diplopia, ptosis, dysphonia, dysarthria, severe dysphagia, and respiratory compromise.
Dysphagia and Breathing Difficulties:
Treatment with botulinum toxin products can result in swallowing or breathing difficulties. Patients with pre-existing swallowing or breathing difficulties may be more susceptible to these complications. In most cases, this is a consequence of weakening of muscles in the area of injection that are involved in breathing or swallowing. Deaths as a complication of severe dysphagia have been reported after treatment with botulinum toxin. Dysphagia may persist for several months, and require use of a feeding tube to maintain adequate nutrition and hydration. Aspiration may result from severe dysphagia and is a particular risk when treating patients in whom swallowing or respiratory function is already compromised. Treatment with botulinum toxins may weaken neck muscles that serve as accessory muscles of ventilation. This may result in a critical loss of breathing capacity in patients with respiratory disorders who may have become dependent upon these accessory muscles. There have been postmarketing reports of serious breathing difficulties, including respiratory failure. Patients treated with botulinum toxin may require immediate medical attention should they develop problems with swallowing, speech or respiratory disorders. These reactions can occur within hours to weeks after injection with botulinum toxin.
Pre-existing Conditions at the Injection Site:
Caution should be used when botulinum toxin treatment is used in the presence of inflammation at the proposed injection site(s), ptosis, or when excessive weakness or atrophy is present in the targeted muscle(s). This also applies to patients who have marked facial asymmetry, excessive dermatochalasis, deep dermal scarring, thick sebaceous skin, or when subjects do not respond to 20 Units of botulinum toxin (e.g., the inability to substantially lessen glabellar lines even by physically spreading them apart). Use caution when administering to patients with surgical alterations to the facial anatomy. Do not exceed the recommended dosage and frequency of administration.
Corneal Exposure and Ulceration:
This may require protective drops, ointment, or closure of the eye by patching or other means. Because of its anticholinergic effects, botulinum toxin should be used with caution in patients at risk of developing narrow angle glaucoma. To prevent ectropion, botulinum toxin products should not be injected into the medial lower eyelid area. Ecchymosis easily occurs in the soft tissues of the eyelid. Immediate gentle pressure at the injection site can limit that risk.
Ophthalmic Adverse Reactions:
Dry Eye:
Dry eye has been reported with the use of botulinum toxin products in the treatment of glabellar lines. Reduced tear production, reduced blinking, and corneal disorders may occur with use of botulinum toxins. If symptoms of dry eye (e.g., eye irritation, photophobia, or visual changes) persist, consider referring the patient to an ophthalmologist.
Spatial Disorientation and Double Vision Treated for Strabismus:
Inducing paralysis in one or more extraocular muscles may produce spatial disorientation, or double vision.. Covering the affected eye may alleviate these symptoms.
Human Albumin and Transmission of Viral Diseases:
The product contains albumin, a derivative of human blood. Based on effective donor screening and product manufacturing processes, it carries an extremely remote risk for transmission of viral diseases and variant Creutzfeldt-Jakob disease (vCJD). There is a theoretical risk for transmission of Creutzfeldt-Jakob disease (CJD), but if that risk actually exists, the risk of transmission would also be considered extremely remote. No cases of transmission of viral diseases, CJD or vCJD have ever been identified for licensed albumin or albumin contained in other licensed products.
Facial Anatomy in the Treatment of Glabellar Lines:
Caution should be exercised when administering botulinum toxin to patients with surgical alterations to the facial anatomy, excessive weakness or atrophy in the target muscle(s), marked facial asymmetry, inflammation at the injection site(s), ptosis, excessive dermatochalasis, deep dermal scarring, thick sebaceous skin, or the inability to substantially lessen glabellar lines by physically spreading them apart. Do not exceed the recommended dosage and frequency of administration. In clinical trials, subjects who received a higher dose had an increased incidence of eyelid ptosis.
Intradermal Immune Reaction:
The possibility of an immune reaction when injected intradermally is unknown. The safety of botulinum toxin for the treatment of hyperhidrosis has not been established. It is approved only for intramuscular injection.
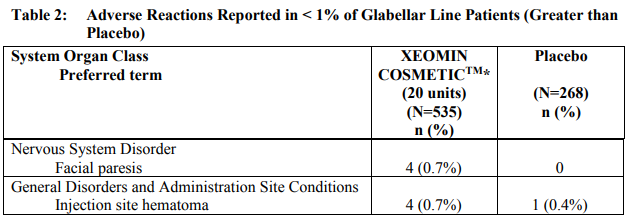
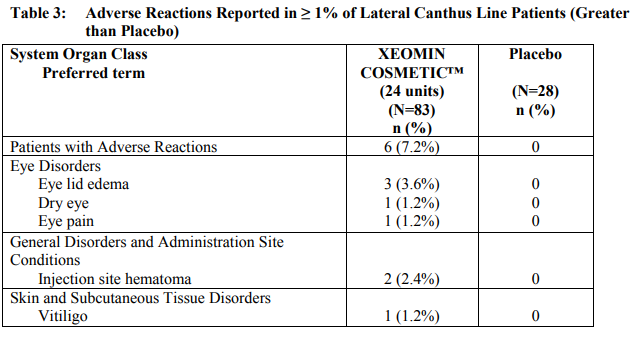
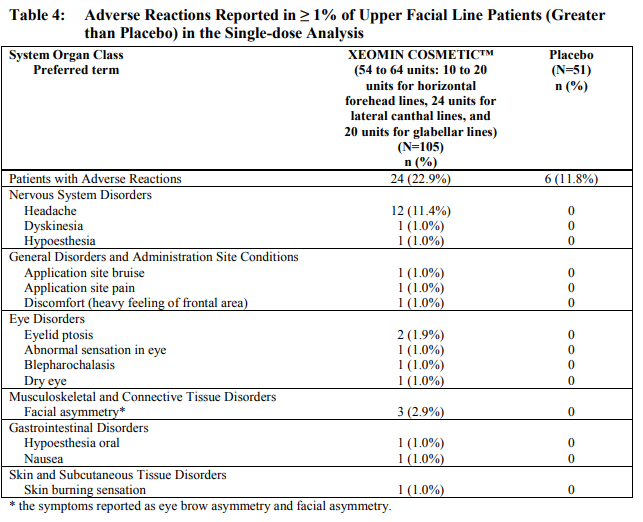
Side Effects/ Adverse Reactions
Here is the list of major side effects taken from the Xeomin, botulinum toxin. Most botulinum toxin share similar side effect / adverse event profile. Please check your package insert for a detailed list.

Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to botulinum toxin in different studies or to other products may be misleading.
Treatment with botulinum toxins may result in the formation of neutralizing antibodies that may reduce the effectiveness of subsequent treatments by inactivating the biological activity of the toxin. The critical factors for neutralizing antibody formation have not been well characterized. The results from some studies suggest that botulinum toxin injections at more frequent intervals or at higher doses may lead to a greater incidence of antibody formation. The potential for antibody formation may be minimized by injecting with the lowest effective dose given at the longest feasible intervals between injections.
Post Marketing Experience
Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. The following adverse reactions have been identified during post-approval use of botulinum toxin products:
Death, sometimes associated with dysphagia, pneumonia, and/or other significant debility or anaphylaxis.
Adverse events involving the cardiovascular system, including arrhythmia and myocardial infarction, some with fatal outcomes. Some of these patients had risk factors including cardiovascular disease.
New onset or recurrent seizures, typically in patients who are predisposed to experiencing these events.
Ear and labyrinth disorders: Hypoacusis; tinnitus; vertigo.
Eye disorders: Diplopia; dry eye; lagophthalmos; strabismus; visual disturbances; vision blurred.
Gastrointestinal disorder: Abdominal pain; diarrhea; dry mouth; nausea; vomiting.
General disorders and administration site conditions: Denervation; malaise; pyrexia.
Metabolism and nutrition disorders: Anorexia.
Musculoskeletal and connective tissue disorders: Localized muscle twitching/involuntary muscle contractions; muscle atrophy; myalgia.
Nervous system disorders: Brachial plexopathy; dysarthria; facial palsy; hypoaesthesia; localized numbness; myasthenia gravis; paresthesia; peripheral neuropathy; radiculopathy; syncope.
Respiratory, thoracic and mediastinal disorders: Aspiration pneumonia; dyspnea; respiratory depression and/or respiratory failure.
Skin and subcutaneous tissue disorders: Alopecia, including madarosis; hyperhidrosis; pruritus; skin rash (including erythema multiforme, dermatitis psoriasiform, and psoriasiform eruption).
Vertigo, photophobia, influenza-like illness, amyotrophy, burning sensation, facial paresis, hypoesthesia, erythema, dry eye, and excessive granulation tissue.
Hypersensitivity reactions including anaphylaxis.
Eye swelling, eyelid edema, dysphagia, nausea, flu-like symptoms, injection site pain, injection site reaction, allergic dermatitis, localized allergic reactions like swelling, edema, erythema, pruritus or rash, herpes zoster, muscular weakness, muscle spasm, dysarthria, myalgia and hypersensitivity.
Drug Interactions
Aminoglycosides and Other Agents Interfering with Neuromuscular Transmission: Co-administration of botulinum toxin and aminoglycosides or other agents interfering with neuromuscular transmission (e.g., curare-like compounds or tubocurarine-type muscle relaxants) should only be performed with caution as the effect of the toxin may be potentiated. If co-administered, the patient should be observed closely.
Anticholinergic Drugs: Use of anticholinergic drugs after administration of botulinum toxin may potentiate systemic anticholinergic effects such as blurred vision.
Other Botulinum Neurotoxin Products: The effect of administering different botulinum neurotoxin products at the same time or within several months of each other is unknown. Excessive neuromuscular weakness may be exacerbated by administration of another botulinum toxin prior to the resolution of the effects of a previously administered botulinum toxin.
Muscle Relaxants: Excessive weakness may also be exaggerated by administration of a muscle relaxant before or after administration of botulinum toxin.
Specific Populations
Pregnancy: There are no adequate data from postmarketing surveillance on the developmental risk associated with the use of botulinum toxin in pregnant women. In animal studies, administrations of botulinum toxin during pregnancy resulted in adverse effects on fetal growth (decreased fetal body weight and skeletal ossification) at clinically relevant doses, which were associated with maternal toxicity.
Lactation: There are no data on the presence of botulinum toxin in human or animal milk, the effects on the breastfed child, or the effects on milk production. The developmental and health benefits of breastfeeding should be considered along with the mother’s clinical need for botulinum toxin and any potential adverse effects on the breastfed infant from botulinum toxin or from the underlying maternal conditions.
Pediatric Use: Safety and effectiveness in patients below the age of 18 years have not been established for botulinum toxin.
Geriatric Use: In clinical studies of botulinum toxin, the responder rates appeared to be higher for subjects younger than age 65 than for subjects 65 years or older. However, no overall differences in safety or effectiveness were observed between older and younger patients. Other clinical studies have not identified differences in responses between older and younger patients, but increased sensitivity in older patients cannot be ruled out.
Females and Males of Reproductive Potential: In rats, botulinum toxin produced adverse effects on mating behavior and fertility.
Ethnic Groups: Exploratory analyses in trials for glabellar lines in African-American subjects with Fitzpatrick skin types IV, V, or VI and in Hispanic subjects suggested that response rates at Day 30 were comparable to and no worse than the overall population.
Overdose
Excessive doses of botulinum toxin, whether it’s BOTOX Cosmetic (onabotulinumtoxinA), DYSPORT, XEOMIN, JEUVEAU (prabotulinumtoxinAxvfs), or DAXXIFY, may be expected to produce neuromuscular weakness with a variety of symptoms. Symptoms of overdose are likely not to be present immediately following injection.
Should accidental injection or oral ingestion occur, or overdose be suspected, these patients should be considered for further medical evaluation and appropriate medical therapy immediately instituted, which may include hospitalization. The person should be medically supervised for several weeks for signs and symptoms of systemic muscular weakness which could be local, or distant from the site of injection.
In the event of overdose, antitoxin raised against botulinum toxin is available from the Centers for Disease Control and Prevention (CDC) in Atlanta, GA. However, the antitoxin will not reverse any botulinum toxin-induced effects already apparent by the time of antitoxin administration.
In the event of suspected or actual cases of botulinum toxin poisoning, please contact your local or state Health Department to process a request for antitoxin through the CDC.
Clinical Pharmacology
Mechanism of Action
The mechanism of action of botulinum toxin involves several steps:
1. Binding: The botulinum toxin binds to specific surface receptors on nerve endings. This binding is facilitated by the heavy chain of the toxin molecule.
2. Internalization: Once bound, the toxin is internalized into the nerve terminal through a process known as receptor-mediated endocytosis.
3. Inhibition of Acetylcholine Release: Inside the nerve terminal, the toxin cleaves a pre-synaptic protein called SNAP-25. This protein is integral to the successful docking and release of acetylcholine, a neurotransmitter responsible for muscle contraction, from vesicles situated within nerve endings. The cleavage of SNAP-25 inhibits the release of acetylcholine, leading to a localized reduction in muscle activity.
4. Muscle Response: The affected muscle undergoes partial chemical denervation, which may lead to muscle atrophy. These changes contribute to the muscle’s reduced activity and the wrinkle smoothing.
The effects of botulinum toxin are not permanent. Over time, the muscle begins to regain its strength through a process known as reinnervation. This occurs as the neuromuscular junction recovers from SNAP-25 cleavage and new nerve endings are formed. The parent nerve terminal regains function, and the collateral terminals, which had sprouted during the period of denervation, retract. This gradual recovery of muscle function ensures the safety of botulinum toxin use in cosmetic medicine, as the effects can be reversed over time.
Pharmacodynamics:
No formal pharmacodynamic studies have been conducted with these toxins. The primary pharmacodynamic effect is due to chemical denervation of the treated muscle resulting in a measurable decrease of the compound muscle action potential, causing a localized reduction in muscle activity. The return of increased muscle tone following injection typically occurs within 3 to 4 months.
Pharmacokinetics:
Using currently available analytical technology, it is not possible to detect these toxins in the peripheral blood following intramuscular injection at the recommended doses.
Carcinogenesis, Mutagenesis, Impairment of Fertility:
Long term studies in animals have not been performed to evaluate carcinogenic potential of these toxins. They were negative in a battery of in vitro and in vivo genetic toxicologic assays. In fertility studies, reduced fertility was observed in males and females at high doses.
Patient Consultation
The patient consultation is a critical component of a successful botulinum toxin treatment. It provides an opportunity to understand the patient’s concerns, set realistic expectations, and plan the treatment accordingly.
Initial Consultation
1. Patient History: Begin with a comprehensive history, including medical conditions, previous cosmetic procedures, allergies, and medications. This information is crucial to assess the suitability of botulinum toxin treatment and to anticipate potential complications.
2. Informed Consent: Explain the procedure, potential risks, benefits, and alternatives to the patient. Ensure they understand the information and have the opportunity to ask questions. Obtain written consent before proceeding with the treatment.
3. Photographic Documentation: Take standardized ‘before’ photographs from multiple angles. These photos serve as a reference for treatment planning and to evaluate the treatment outcome.
Patient Examination
1. Patient Concerns: Provide a mirror and ask the patient to point out the areas of concern. Ask them to animate their face to illustrate their concerns better. This step helps to understand the patient’s perception of their appearance and their aesthetic goals.
2. Facial Analysis: Conduct a thorough examination of the face, noting asymmetries, skin quality, muscle strength, and the depth and location of wrinkles. Point out any asymmetries to the patient and document them in the medical record.
3. Glogau Wrinkle Scale: Use the Glogau Wrinkle Scale to assess the severity of wrinkles. This scale categorizes wrinkles into four types, each associated with a specific age group and recommended treatment:
– Type 1: ‘Early Wrinkles’ (20s to 30s) – botulinum toxin is typically sufficient.
– Type 2: ‘Wrinkles in Motion’ (30s to 40s) – botulinum toxin and possibly dermal fillers may be needed.
– Type 3: ‘Wrinkles at Rest’ (50s & older) – botulinum toxin and dermal fillers will likely be required.
– Type 4: ‘Only Wrinkles’ (60s or 70s) – botulinum toxin and dermal fillers may not be enough; consider facelift or laser resurfacing.
4. Glabellar Spread Test: This test helps determine if botulinum toxin alone will soften a patient’s frown lines. Spread the glabellar wrinkles apart with your thumb and index fingers. Patients with thick skin and deep dermal folds who do not improve with manual spreading may need dermal filler injections alongside botulinum toxin.
Setting Expectations
1. Realistic Expectations: Discuss the expected outcomes and limitations of botulinum toxin treatment. Emphasize that the typical goal is to enhance their natural beauty and not to completely change their appearance.
2. Patient Education: Educate the patient about the procedure, post-treatment care, and the need for follow-up sessions. Explain that the effects of botulinum toxin are temporary and regular treatments are necessary to maintain the results.
3. Treatment Plan: Based on the patient’s concerns, facial analysis, and wrinkle assessment, develop a personalized treatment plan. Discuss the plan with the patient, including the areas to be treated, the type of botulinum toxin to be used, and the estimated cost.
The patient consultation is not just about gathering information but also about building a therapeutic relationship with the patient. A well-conducted consultation can lead to high patient satisfaction and a successful treatment outcome.
Counseling
Patients should be informed that injections of botulinum toxins, such as BOTOX Cosmetic, DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY, may lead to potential swallowing, speaking, or breathing difficulties, or other unusual symptoms. If such symptoms develop or existing symptoms worsen, patients or caregivers should seek immediate medical care.
Patients should also be aware that these injections may cause eye dryness, and they should report any symptoms of eye dryness, such as eye pain, eye irritation, photosensitivity, or changes in vision, to their doctor.
In addition, patients should be advised to avoid driving a car or engaging in other potentially hazardous activities if they experience loss of strength, muscle weakness, blurred vision, or drooping eyelids.
It’s important to note that these are general guidelines and the specific details may vary between the different toxins. Always refer to the specific patient counseling information for each toxin for the most accurate information.
Injecting the Glabella/Procerus and Corrugator Muscle
The glabellar region, often referred to as the ‘frown lines,’ is a common area for botulinum toxin injections. The primary muscles involved in this region are the procerus and corrugator muscles.
Muscles Involved and Action
1. Procerus: This muscle originates from the nasal bone and inserts into the medial forehead and skin of the brow. Its action is to draw the medial brow inferiorly, contributing to the horizontal lines seen on the forehead.
2. Corrugator: The corrugator muscle originates from the medial superciliary arch and inserts into the skin of the medial forehead. It draws the brow medially and inferiorly, leading to the formation of vertical lines between the eyebrows.
Landmarks
Identifying the correct landmarks is crucial for successful injections. Here are the key landmarks for glabellar injections:
1. Medial Corrugator: The injection should be 1 cm above the bony orbital rim and vertical to the medial canthus.
2. Lateral Corrugator: The injection should be 1 cm above the bony orbital rim and medial to the vertical mid-pupillary line.
3. Procerus: The injection should be just above the crossing point of the ‘X’ formed by drawing a line from the medial eyebrow contralateral to the medial canthus.
Injection Technique
All injections for the glabella are intramuscular and perpendicular to the skin. The needle should be above the periosteum. It’s important to note that the frontalis muscle overlaps the corrugator superficially, so a superficial injection may cause paralysis of the inferior edges of the frontalis muscle. Therefore, corrugator injections should be deep intramuscular injections.
Previously, the recommendation was to inject until hitting the periosteum, then pull back several millimeters before injecting the botulinum toxin. However, this technique has been modified as it was found to increase the incidence of headaches in patients and dull the needle for subsequent injections.
The standard FDA-approved dose for glabellar lines, as per the BOTOX® Cosmetic package insert, is 20 units. However, men may require an additional 1-2 units per injection site due to typically larger muscle mass.
Complications and Solutions
The complication rate for glabellar injections is 1-3%. Potential complications include:
1. Lid Ptosis: This can occur if the injection is too close to the orbital rim, as diffusion of the botulinum toxin may affect the levator palpebrae superioris muscle.
2. Brow Ptosis: This can occur if the injection is placed too superficially (affecting the frontalis muscle) or too lateral to the mid-pupillary line.
Complications can appear as soon as 48 hours or as late as 7 days post-injection and may persist for 4-8 weeks. Solutions include:
1. Lid Ptosis: Apraclonidine 0.5% drop can be used, one drop to the affected eye three times a day. This stimulates Mueller’s muscles to minimize the ptosis. Oxymetazoline 0.1%, which has the FDA approval for lid ptosis, can also be used.
2. Brow Ptosis: A brow lift injection technique can be attempted. However, typically, time is required for frontalis movement to reappear to lift the brow up once again.
Injecting the Brow for a Brow Lift
Injections above near the brows that paralyzes the depressor muscles and create a “brow lift” like effect.
Muscles Involved and Action
The primary muscles involved in a brow lift procedure using botulinum toxin are the Procerus and the Orbicularis Oculi.
Procerus
The Procerus muscle originates from the nasal bone and inserts into the medial forehead and skin of the brow. Its primary action is to draw the medial brow inferiorly, contributing to the formation of horizontal wrinkles on the bridge of the nose.
Orbicularis Oculi
The Orbicularis Oculi is a circumferential muscle group that functions like a sphincter or a purse string. It originates from the medial palpebral ligament and inserts into the lateral palpebral raphe, corrugator, frontalis, and depressor supercilii. Its action pulls the skin of the forehead, temple, and cheek toward the medial angle of the orbit, and it is also responsible for closing the eyelids.
Landmarks
The key landmarks for a brow lift procedure are the crossing point of the X formed by drawing a line from the medial eyebrow contralateral to the medial canthus for the Procerus, and the superolateral portion of the Orbicularis Oculi as it curves infralaterally lateral to the temporal fusion line for the Orbicularis Oculi.
Injection Technique
Procerus
The Procerus should receive a deep intramuscular injection, just above the periosteum. Inject 4 units of botulinum toxin to the Procerus just above the crossing point of the X formed by drawing a line from the medial eyebrow contralateral to the medial canthus.
Orbicularis Oculi
For the Orbicularis Oculi, inject 3 units subcutaneously to the superolateral portion of the muscle as it curves infralaterally lateral to the temporal fusion line. Ensure that the movement of the lateral portions of the frontalis muscles is not felt in this superolateral injection site to avoid injecting the frontalis and creating brow ptosis. The injection should be placed 1 cm outside of the bony orbital rim.
Complications and Solutions
The primary complication of a brow lift procedure is brow ptosis, or drooping of the brow. This can be minimized by injecting superior and lateral to the orbital rim. If brow ptosis does occur, it will naturally resolve as the action of the botulinum toxin diminishes over time.
Additional Pearls
– Precise injection location and depth are crucial for achieving aesthetically pleasing brow outcomes and greater duration of efficacy.
– Avoiding the frontalis muscle during injection is key to prevent brow ptosis.
– Always consider individual patient anatomy when planning and executing the procedure.
Injecting the Horizontal Forehead Lines or Frontalis Muscle
The primary indication for injecting the frontalis muscle is to reduce the appearance of horizontal forehead lines. These lines are a result of the repetitive contraction of the frontalis muscle, which lifts the eyebrows and furrows the forehead.
Muscles Involved and Action
The frontalis muscle is a broad muscle that varies in size and shape among individuals. Some may have a narrow or broad frontalis, while others may have a tall or short frontalis. The shape can also vary, being either V-shaped or rectangle-shaped. It is important to palpate the muscle before injecting to understand its size and shape.
The frontalis muscle originates from the galea aponeurosis and inserts into the muscles of the glabellar complex. The action of the frontalis muscle is to lift the eyebrows superiorly and depress the scalp inferiorly. The fibers of the frontalis muscles are oriented vertically, while the visible wrinkles formed by the contraction of the frontalis muscle are horizontal.
Landmark
The frontalis muscle is located on the forehead and is easily palpable. The lower 2-3 cm of the frontalis muscle is used to elevate the eyebrow and injection here should be avoided. The medial portions of the frontalis muscle fibers may be more fibrous or absent and may need less injection. A key point about the frontalis is to avoid injecting near the lowest horizontal wrinkle or at least 2-3 cm above the brow.
Injection Technique
The injections are subcutaneous and are typically placed roughly 2 cm apart. Typically, 2 units of botulinum toxin are injected per site. Men may require 1-2 additional units per injection site due to typically having a larger muscle mass.
Complications and Solutions
The most common complications associated with frontalis muscle injections include brow ptosis and Spock brow.
Brow ptosis: This can occur when the frontalis is treated without paralyzing the active brow depressor muscles (procerus and corrugator). Ideally, glabella muscles should be injected simultaneously. Another cause of brow ptosis is when the frontalis muscle, which is hyperfunctional, supports a normally ptotic upper eyelid. To avoid complete paralysis of the frontalis muscle, it is recommended to avoid injecting near the first horizontal line or at least 2-3 cm above the brow.
Spock brow: This can occur when the lateral fibers of the frontalis muscles have not been paralyzed. The solution is to inject 1-2 units where you feel the untreated lateral fibers of the frontalis muscle when you ask your patients to lift their eyebrows. It should be noted that some patients may actually prefer the “Spock brow” look.
Additional Pearls
1. Always palpate the frontalis muscle before injecting to understand its size and shape. This will help in determining the amount of botulinum toxin needed and the best injection sites.
2. Always avoid injecting near the lowest horizontal wrinkle line or at least 2-3 cm above the brow to prevent brow ptosis.
3. When treating the frontalis muscle, consider also treating the glabella muscles to prevent brow ptosis.
4. Be aware of the possibility of a Spock brow and know how to correct it if it occurs.
Injecting the Crow’s Feet or Orbicularis Oculi
Muscles Involved and Action
The orbicularis oculi is a single, circumferential muscle group that functions like a sphincter or purse string. The muscle originates from the medial palpebral ligament and inserts into the lateral palpebral raphe, corrugator, frontalis, and depressor supercilii. Its primary action involves pulling the skin of the forehead, temple, and cheek toward the medial angle of the orbit, resulting in the closure of the eyelids.
Landmark
The landmark for the injection is 1 cm outside of the bony orbital rim or 2 cm outside of the lateral cantus. Placing the non-injecting index finger into the bony rim can help identify this landmark. The injection site should not be below the zygomatic arch to avoid diffusion into the zygomatic muscles, which can affect the smile.
Injection Technique
The injection technique for the orbicularis oculi involves subcutaneous injections, typically 1 cm apart in a slightly curving arch. Each injection typically contains 3 units of botulinum toxin. Men may require an additional 1 unit per injection site due to their typically thicker skin and stronger muscle mass.
Complications and Solutions
The most common complications include asymmetrical smile or diplopia due to migration of the toxin. To avoid this, it is crucial to inject 1 cm outside of the bony orbital rim. Excessive wrinkles underneath the lower lid may become accentuated if medial portions of the Orbicularis Oculi are left unopposed. This may require injection into the lower/medial parts of the Orbicularis Oculi or the Nasalis muscle.
Injecting the Lower Eyelid
Botulinum toxin injections in the lower eyelid are primarily indicated for the treatment of wrinkles below the lower eyelid and narrow palpebral aperture.
Muscles Involved
The primary muscle involved in this procedure is the Orbicularis Oculi. This muscle is a circumferential muscle group that functions like a sphincter or purse string. It originates from the medial palpebral ligament and inserts into the lateral palpebral raphe, corrugator, frontalis, and depressor supercili. Its action pulls the skin of the forehead, temple, and cheek toward the medial angle of the orbit, and it is responsible for closing the eyelids.
Injection Technique
The injection technique for the lower eyelid involves a subcutaneous injection of botulinum toxin. The standard dose is 1 unit, injected 0.5 cm below the lower lid margin in line with the midpupillary line. Some individuals may require an additional unit for optimal results. It is important to avoid injections medial to the pupil to minimize the risk of complications.
Complications
The most common complication of lower eyelid injections is bruising, as this is a vascular area. Other potential complications include ectropion, where the lower lid turns outwards, and epiphora, which is excessive tear production. These complications are extremely rare but can occur.
To minimize the risk of ectropion, it is crucial to select patients appropriately. Patients with a history of lower lid ablative resurfacing or blepharoplasty may be contraindicated. Even in the absence of these contraindications, it is recommended to perform a snap test before proceeding with the injection. This test involves pulling the lower eyelid downward; a return to its normal position in less than 1 second is considered normal. Any patient with a time greater than 1 second should not be treated.
Injecting the Nasalis/Bunny Nose Lines
Muscles Involved and Action
The primary muscles involved in the formation of bunny nose lines are the Nasalis and Procerus muscles. Treatment of both the Procerus and Nasalis is necessary to diminish the horizontal and vertical lines on the bridge of the nose.
The Nasalis muscle, originating in the maxilla, is a complex structure that inserts into the aponeurosis of the Procerus and continues over the bridge of the nose onto the other side. Its primary function is to draw the skin of the nose superiorly and medially. Procerus muscle, which originates from the nasal bone, inserts into the medial forehead and skin of the brow. Its primary function is to draw the medial brow inferiorly.
Landmarks
When it comes to injecting these muscles, accurate identification of the landmarks is crucial. For the Nasalis, the injection site is anterior and medial to the nasofacial groove on the lateral nose. For the Procerus, the injection is performed just above the crossing point of the X formed by drawing a line from the medial eyebrow contralateral to the medial canthus.
Injection technique
The Procerus requires a deep intramuscular injection, above the periosteum, with an injection of 4 units at the identified landmark. The Nasalis, on the other hand, requires a subcutaneous injection, with 2 units injected at the landmark.
Complications
One potential complication is upper lip ptosis due to diffusion into muscles lateral to the Nasalis muscle. To avoid this, ensure the injection is performed medial and anterior to the nasofacial groove, thus avoiding the levator muscles of the lip.
Injecting the Lip for a Lip Flip
Muscles Involved and Action
The primary muscle involved in the lip flip procedure is the orbicularis oris muscle. This muscle encircles the mouth and is responsible for various lip movements, including closing the lips, puckering, and other complex movements necessary for speech and facial expression.
When botulinum toxin is injected into the orbicularis oris muscle, it causes a temporary paralysis of the muscle. This results in a slight eversion or ‘flip’ of the lip, giving the appearance of a fuller and more pronounced upper lip.
Landmark
The landmark for the lip flip procedure is the vermilion border of the upper lip. The vermilion border is the line where the pink-red lip tissue meets the surrounding skin. The injections are typically placed along this border at several points across the upper lip.
Injection Technique
The injection technique for a lip flip involves the careful placement of 1-2 units into the orbicularis oris muscle. The injections are typically administered using a fine needle, and the procedure is usually performed without anesthesia as it causes minimal discomfort.
The injections are placed along the vermilion border of the upper lip, typically at 2-3 points on each side of the midline. The exact number and placement of injections can vary depending on the individual patient’s anatomy and desired results.
Complications and Solutions
Complications from a lip flip procedure are generally rare and mild, but can include:
– Asymmetry: This can occur if the botulinum toxin is not evenly distributed on both sides of the lip. It can be corrected in a follow-up appointment with additional injections to balance the effect.
– Difficulty with lip movements: Over-paralysis of the orbicularis oris muscle can lead to difficulty with certain lip movements, such as puckering or drinking from a straw. This is usually temporary and resolves as the effect wears off.
– Bruising or swelling at the injection site: This is a common side effect of any injection and usually resolves on its own within a few days.
Additional Pearls
– The effect of the lip flip procedure is temporary, with muscle function typically beginning to return approximately 1 to 2 months after injection due to the low dosage.
– The lip flip procedure can be a good alternative for patients who want a more pronounced upper lip but do not want or are not ready for more invasive procedures such as fillers or surgery.
– It’s important to have a thorough understanding of the patient’s anatomy and desired outcome to achieve the best results with a lip flip procedure.
– Patient education is key. Make sure patients understand that the results are subtle and that this procedure is different from a dermal filler injection.
Injecting the Orbicularis Oris / Smoker’s Lip Lines
Muscles Involved and Action
The primary muscle involved in this procedure is the Orbicularis Oris. This muscle originates from the buccinator and fibers at the angle of the mouth, and inserts symmetrically at the vermillion border. The primary action of the Orbicularis Oris is to close the lips, which is crucial for functions such as speaking, eating, and expressing emotions.
Landmark
The Orbicularis Oris is a complex muscle that encircles the mouth. It is located directly beneath the skin and is easily palpable. The vermillion border of the lips serves as a key landmark for this muscle. The muscle extends from the corners of the mouth and wraps around the lips, meeting at the midline.
Injection Technique
The injection technique for the Orbicularis Oris involves subcutaneous symmetrical injections less than 3 mm above and below the vermillion border. Each injection should contain 1-2 units of botulinum toxin. It is important to avoid injecting more than 2 units in each lip quadrant to prevent overcorrection and potential complications.
The mid upper lip and the corners of the mouth should be avoided during the injection process. The mid upper lip is a sensitive area, and injecting it could lead to flattening of the lip. The corners of the mouth are also crucial for facial expressions, and injecting them could lead to an asymmetrical smile or other complications.
Complications and Solutions
Potential complications of botulinum toxin injections in the Orbicularis Oris include an asymmetrical smile, difficulty with speech, and drooling. These complications can be mitigated by using a low dose of botulinum toxin and ensuring symmetrical injections.
It is also recommended to avoid injecting individuals who rely heavily on their facial expressions for their profession, such as singers, orators, and musicians. These individuals may experience a significant impact on their ability to perform their work if any complications arise.
If a patient has a history of cold sores, it is recommended to include pretreatment with Valtrex®. The patient should take 2 grams at the time of treatment and 2 grams 12 hours later to prevent a herpes outbreak.
Additional Pearls
Patient Selection: It is crucial to select patients carefully for this procedure. Patients deep peri-oral grooves may benefit from laser resurfacing, microneedling or dermal filler injection.
Dysport: Introduction and Differences from Botox
Dysport requires an explanation, because the units are different from other botulinum toxins. All package inserts state that units are not interchangeable with other preparations of botulinum toxin products. However, most commercially available botulinum toxins use 20 units for the glabellar line. Except for Dysport. Units are a measure of the biological activity of a botulinum toxin which cannot be compared to nor converted into units of any other botulinum toxin products assessed with any other specific assay method.
Reconstitution
Dysport is supplied as a single-use vial with 300 Units per vial. Each 300 Unit vial of Dysport is to be reconstituted with 2.5 mL of 0.9% sterile, preservative-free saline prior to injection. The concentration of the resulting solution will be 10 Units per 0.08 mL. Each 300 Unit vial of Dysport may also be reconstituted with 1.5 mL 0.9% sterile, preservative-free saline for a solution of 10 Units per 0.05 mL to be delivered. Just as a provider can dilute Botox Cosmetic with Preserved (Bacteriostatic) 0.9% Sodium Chloride, Dysport may also be diluted with the same to increase its half-life.
Unit Conversion from Botox Cosmetic to Dysport
The striking difference between Dysport and Botox Cosmetic is the amount of units injected. Botox Cosmetic requires 20 units at 4 units per injection site in treating the glabellar area, whereas Dysport requires 50 units at 10 units per injection site in treating the glabellar area. This constitutes a 1:2.5 concentration ratio. Many other users have contended that the actual ratio should be 1:3 or 1:4. These concentrations ultimately increase the amount of Dysport being injected. We recommend that you start with a 1:2.5 ratio conversion from the Botox Cosmetic unit injection recommendations offered at this course until you feel comfortable with the use of Dysport.
Comparative Studies
Studies have shown that Dysport will start working faster than Botox Cosmetic, last longer than Botox Cosmetic, and have a lower diffusion rate than Botox Cosmetic due to its high concentration. However, it’s important to note that individual patient results may vary, and it’s crucial to tailor the treatment plan to the patient’s unique needs and desired outcomes.
In conclusion, Dysport provides an effective alternative to Botox Cosmetic, with its own unique properties and considerations. As with any treatment, understanding the product and its appropriate use is key to achieving optimal results.
Treatment Failure in Botulinum Toxin Cosmetic Injection
One of the most significant challenges is treatment failure, which can be classified into primary and secondary nonresponse.
Primary Nonresponders:
Primary nonresponders are individuals who do not respond to their first BTX Cosmetic treatment. This lack of response can be attributed to several factors:
1. Static Wrinkles: The most common reason for primary nonresponse is the presence of static wrinkles, which are not dynamic in origin. These wrinkles are usually due to photodamage or age-related changes and require the injection of a filler material. A positive spread test often indicates this.
2. Inadequate Injection Amount: Another common cause of primary nonresponse is an inadequate amount of BTX injected. This could be due to the patient having strong muscles or the injection missing the targeted muscle.
3. Denatured Toxin: If the BTX has denatured, it will not produce the desired effect. In such cases, contact your representative for a new vial.
Secondary Nonresponders:
Secondary nonresponders are patients who initially respond to BTX Cosmetic but lose the response on subsequent injections. The reasons for this can be:
1. Neutralizing Antibodies: Some patients may develop neutralizing antibodies to BTX. This is a rare side effect, but it has been observed in some patients. In such cases, using a different Botulinum Toxin may yield better results.
2. Inadequate Injection Amount: Similar to primary nonresponse, secondary nonresponse can also be due to an inadequate amount of BTX injected. This could be due to the patient having strong muscles or the injection missing the targeted muscle.
Botulinum Toxin Complications and Treatments for Complications
Localized Complications
Localized complications are those that occur in the immediate area of the injection. These can include:
– Bruising and Bleeding: This is a common complication that can occur due to the puncture of blood vessels during the injection process. It is usually minor and resolves on its own. Applying a cold compress to the area immediately after the injection can help reduce bruising and swelling. Over-the-counter pain relievers can also be used to manage any discomfort.
– Pain and Swelling: Some patients may experience pain and swelling at the injection site. This is typically transient and can be managed with over-the-counter pain relievers and cold compresses.
– Infection: Although rare, infections can occur if the injection site is not properly cleaned before the procedure. If an infection is suspected, it should be treated promptly with antibiotics.
Systemic Complications
Systemic complications are those that affect the entire body or multiple body systems. These can include:
– Botulism: This is a rare but serious complication that can occur if the toxin spreads beyond the injection site. Symptoms can include muscle weakness, difficulty swallowing, and respiratory problems. If suspected, immediate medical attention is required. If botulism is suspected, the patient should be hospitalized immediately. Antitoxin therapy should be initiated as soon as possible to neutralize the toxin.
– Allergic Reactions: Some patients may have an allergic reaction to the BTX. Symptoms can include hives, difficulty breathing, and swelling of the face, lips, tongue, or throat. If an allergic reaction occurs, the patient should be treated with epinephrine and antihistamines. In severe cases, hospitalization may be necessary.
Managing Lid Ptosis Complication and Treatment
Lid ptosis, or drooping of the upper eyelid, is a potential complication of botulinum toxin injections. It can occur when the toxin diffuses into the levator palpebrae superioris muscle, which is responsible for lifting the eyelid. This can lead to an undesirable aesthetic outcome and, in severe cases, can interfere with vision.
The management of lid ptosis following botulinum toxin injection involves both preventive and corrective measures.
Preventive Measures
1. Accurate Injection Technique: The most effective way to prevent lid ptosis is to ensure accurate injection technique. This includes proper identification of the injection site, avoiding the levator palpebrae superioris muscle, and injecting the toxin at a safe distance from the eyelid.
2. Patient Positioning: The patient should be in an upright position during the injection and for 3-4 hours post-injection. This helps to minimize the diffusion of the toxin.
3. Patient Instructions: Patients should be instructed to avoid rubbing or massaging the injection area for at least 24 hours post-injection to prevent the spread of the toxin.
Corrective Measures
1. Alpha-adrenergic eye drops: In the event of lid ptosis, alpha-adrenergic eye drops such as apraclonidine 0.5% can be used. Oxymetazoline, Upneeq, 0.1% has been FDA approved for the treatment of eyelid ptosis. These drops stimulate the Müller muscle, a smooth muscle that assists in elevating the eyelid, thereby providing a temporary lift to the drooping eyelid. These drops can be used until the ptosis resolves.
Naphcon-A, Naphazoline/Pheniramine, is another over the counter option. This class of drug is known as sympathomimetic amines. There are no comparative clinical trials examining the benefits of any of the medications with each other.
2. Wait for Toxin to Wear Off: Botulinum toxin effects are temporary, and the ptosis will resolve naturally as the effects of the toxin wear off, typically within 4-6 weeks.
Pearls in Botulinum Toxin Cosmetic Injection
As health care providers, we are always seeking to refine our skills and improve patient outcomes. This chapter will provide you with valuable insights and pearls of wisdom for administering botulinum toxin injections for cosmetic purposes.
The Power of Touch
The human hand is an incredible tool. Use your hands to feel the face and identify the muscles causing visible wrinkles. This tactile approach will guide you to the precise injection site. Always inject a relaxed face, not a face where the muscle is contracted. Contracted muscles can distort your landmarks and lead to less than optimal results.
Marking the Territory
Until you become proficient, use a marking pen or a white eyeliner pencil to mark your injection sites. However, be sure to place the marks below where you will inject. Injecting into a mark on the face is akin to tattooing someone.
Landmarks: More Than Skin Deep
Many landmarks are bony, not just on the skin’s surface. Do not rely solely on surface skin landmarks as your reference. Understanding the underlying anatomy is crucial for successful injections.
Complications: Be Prepared
Complications can occur as soon as 48 hours or as late as 7 days post-injection and may persist for up to 4 – 8 weeks. Most complications are almost always temporary. In your practice, you are likely to experience a complication. Be prepared for it. Good hand holding and patient reassurance that the complication is temporary will appease most patients. In some cases, offering a money-back refund can eliminate tension and potential headaches.
Documentation: Before and After Photos
Always obtain before and after photos. This is essential documentation to resolve any complaints. It also provides a visual record of the treatment’s effectiveness.
Reinjection: Patience is Key
Reinjection should be done no earlier than one week after the first injection if the patient perceives no desired effect. Sometimes, it takes a week until a patient sees the effects. Patience is key.
Comfort Measures: EMLA and Ice Packs
Application of topical EMLA anesthetic or cold ice pack will help alleviate patient discomfort and injection fears. These simple measures can significantly improve the patient experience.
Pre and Post Injection Instructions
Please become familiar with our standard Pre and Post injection instructions. Your patients will ask you about them. Compliance with these instructions will reduce complications and improve outcomes.
Botulinum Toxin Pricing
Botulinum toxin injections are a significant investment for both the provider and the patient. Understanding the pricing structure is crucial to ensure a profitable practice and to provide clear and transparent information to patients.
Pricing Structure: Per Area, Per Syringe, or Per Unit?
There are different approaches to pricing botulinum toxin injections, and the choice often depends on the provider’s preference and the standard practice in their region. Some practices charge per area or per syringe, often using about 20 units per “area” or “syringe”. However, all manufacturers of botulinum toxin prefer the “per unit” pricing model. This approach provides patients with knowledge of the units they are receiving, promoting transparency and consistency in treatment.
Setting Your Prices
When setting your prices, it’s recommended to research your local market. Call local competitors and inquire about their pricing. If they charge per area, ask how many units they use per area.
As a general guide, here are some typical pricing ranges across the U.S.:
– Dermatologist/Plastic Surgeons: 150-200% higher than manufacturer purchase price
– Average pricing: 100-150% higher than manufacturer purchase price
– Competitive pricing: 75-100% higher than manufacturer purchase price
Remember, these are just guidelines. Your pricing should reflect your expertise, the quality of your service, and your local market conditions.
Legal Considerations
It’s worth noting that purchasing any botulinum toxin products from outside the U.S., such as Canada, is illegal. The FDA has strict regulations on the import of medications, and non-compliance can lead to serious legal consequences.
Additional Pearls
– Transparency is key: Always be upfront with your patients about the cost of their treatment. This includes the number of units they will receive and the total cost.
– Document everything: Keep a record of the number of units used for each patient and each treatment area. This can help you track your usage and costs, and can also be useful in case of any disputes.
– Adjust as needed: Don’t be afraid to adjust your prices as needed based on changes in your costs, market conditions, or the value you provide.
Botulinum Toxin Marketing
Marketing is a crucial aspect of any successful medical practice, and this is especially true for practices offering botulinum toxin injections. The following strategies can help you effectively market your services and attract new patients.
Understanding Your Target Market
Before you begin marketing your services, it’s important to understand who your target market is. Botulinum toxin injections are popular among women aged 35 to 50 years old, but this can vary depending on your location and the specific services you offer. Understanding your target market will allow you to tailor your marketing efforts to the needs and interests of these potential patients.
Branding and Collaboration
Improving the branding of your botulinum toxin services can significantly increase your bookings. This includes creating a professional and appealing logo, using consistent colors and fonts across all marketing materials, and developing a unique selling proposition that sets you apart from competitors.
Collaborating with influencers and local businesses can also be an effective way to drive interest in your services. This could involve partnering with a local fitness center or spa, or working with a popular local blogger or social media influencer to promote your services.
Online Marketing
Having a strong online presence is essential in today’s digital age. This includes having a professional and user-friendly website, as well as active profiles on relevant social media platforms. Search engine optimization (SEO) and pay-per-click (PPC) advertising can also be effective ways to increase your online visibility and attract new patients.
Collecting email addresses from existing patients and using email marketing campaigns can also be a powerful way to keep your services top of mind and encourage repeat bookings.
Traditional Media Advertising
While online marketing is crucial, don’t overlook the potential of traditional media advertising. This could include print ads in local newspapers or magazines, radio ads, or even television commercials. The best platforms for your practice will depend on your target market and local media landscape.
Customer Service and Experience
Providing excellent customer service is crucial for retaining patients and attracting new ones. This includes everything from the initial phone call or email inquiry, to the consultation and treatment process, to follow-up care.
Offering a unique patient experience can also set your practice apart. This could involve offering additional services, such as skincare consultations or massage, or creating a relaxing and luxurious treatment environment.
Education and Promotions
Educating potential patients about the benefits of botulinum toxin injections, and addressing common concerns or misconceptions, can help to build trust and interest in your services.
Offering promotions or discounts can also be an effective way to attract new patients. This could involve offering a discount for first-time patients, or a special promotion for existing patients who refer a friend.
Remember, marketing is not a one-time effort but an ongoing process. Regularly evaluating and adjusting your marketing strategies based on their effectiveness and changes in the market can help to ensure your practice’s success.
For more detailed strategies and tailored advice, consider consulting with our internal marketing specialist or taking advantage of resources offered by botulinum toxin manufacturers.
For more information about Comprehensive Guide to Botulinum Toxin Injection Training, contact us at email@CosmeticMedicalTraining.com or call us at (212) 470-8059.
Statement of Responsibility
Cosmetic Medical Training recognizes that many of the techniques and recommendations are for procedures that are considered off-label use. Our recommendations are based on many textbooks, published articles, seminars, and practical knowledge and experience. The authors have attempted to maintain up to date knowledge and information in this training manual with the current standard of care. However, due to the continuing flow of new research and information relating to the drugs being used in this course, we recommend that you check with the manufacturer for any changes in the package inserts, warnings, and precautions. All information and tools presented within this site are intended for educational purposes. We do not guarantee that the information will be completely accurate and up to date; therefore the authors will not be held responsible for any errors, omissions, or inaccuracies published. Application of the knowledge is ultimately the responsibility of the practitioner.
The owners, authors, and any participants disclaim all liability or loss in conjunction with any content provided here. We disclaim any liability for products or services recommended including defective products or direct, indirect, special, incidental, or consequential damages, arising out of the use or the inability to use the materials/information published.
Originally published at Botox Training St. Louis
